中風的預防及管理
分享到
本文內容針對中風的預防及管理,透過個人的中風風險評估及確保中風後能盡快得到有效的治療,減輕中風帶給家庭及社會的負擔。
完整英文版本已經上載,中文版本即將更新。
中風的預防及管理
減輕中風負擔
這本中風預防和管理文章強調了通過對個人進行中風風險管理篩查以及確保中風發作後迅速有效的治療反應來減輕中風局部負擔的需要。
與其他地方一樣,在香港減輕中風的負擔取決於有效的干預措施,特別是- 通過中風篩查和公眾教育提高公眾對中風的認識,
篩查,評估和干預可改變的中風危險因素;- 持續使用有效的藥物治療;
中風篩查發現期間對任何器質性血管病變採取預防性外科手術或血管內治療於社區裡快速識別中風;和及時有效的急性中風管理.
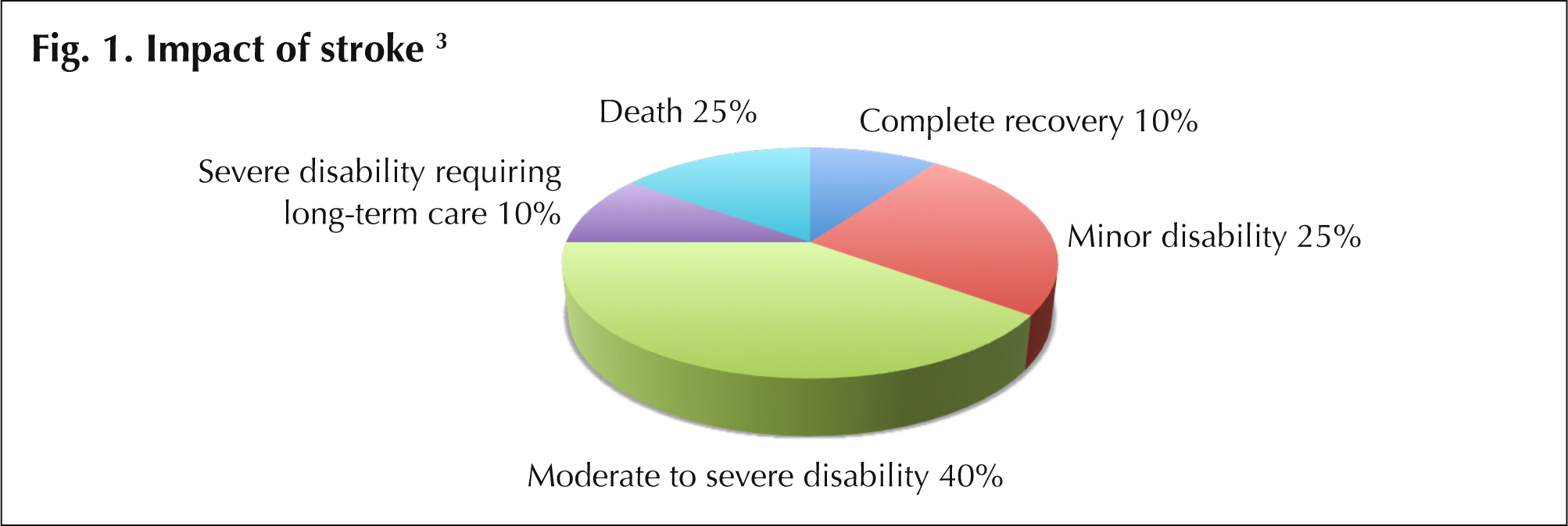
這些主題,尤其是中風預防和急性治療的醫學和外科方面,是本文的重點。但是,人們認識到中風和中風的康復對家庭,看護者和社區的影響更大,而多學科康復是中風倖存者護理的關鍵組成部分。 中風倖存者會經歷各種結果,這些結果取決於他們的年齡,中風的嚴重程度以及治療的成功率和時機[3]。一般的卒中恢復率如圖1所示。 改進的治療方法和更及時的治療方法有可能對個人及其家庭產生積極的影響。
 |
中風篩查
大多數中風是可以預防的,因此預防仍然是減輕個人和廣大社區中風負擔的關鍵[4];可以通過篩查中風的已知危險因素並實施可更改的危險因素管理來實現。在美國,大多數中風中心建議對18歲以上的成年人進行中風篩查。
.
中風的危險因素
表1總結了缺血性中風的危險因素。而表內所顯示的可調節的危險因素代表可以在在生活方式,藥用或手術方面去改善
| Table 1. Risk factors for ischaemic stroke [5,6] | |
| 危險因素(可調較) | |
| • 肥胖 • 吸菸 • 酗酒 • 缺乏運動 • 高血壓 • 糖尿病 • 高膽固醇血症 • 嚴重的頸動脈狹窄 • 顱內動脈狹窄 | •其他顱外或顱內血管異常 |
| 危險因素(非更改) | |
| • 年紀 • 男性 | • 家庭有成員有中風歷史 • 種族 |
INTERSTROKE研究
最近發表的 INTERSTROKE 研究結果使我們對中風的特定風險因素有了更深入的了解。這項研究在全球 22 個國家進行,調查了 3000 例中風病例和 3000 名對照組的缺血性和腦內出血性中風的風險因素。
INTERSTROKE 研究發現,所有中風的十個最重要風險因素是:高血壓、目前吸煙、腰臀比、飲食風險評分、低水平的體力活動、糖尿病、每月攝取超過 30 杯酒或暴飲暴食、心理壓力、抑鬱和心臟病因素。這些風險因素共同解釋了約 90% 的中風風險。
與早期研究一致,INTERSTROKE 研究發現高血壓是所有類型中風最重要的風險因素,對腦內出血性中風的風險因素比缺血性中風更為強大。高血壓在年齡不滿 45 歲的人群中也被證明是一個特別重要的風險因素
在亚洲專科醫生的筛查流程
亞洲醫學專科醫生的篩查是一個全面的過程,包括:
• 對患者進行病史提取和訪談,詢問他們的生活方式、個人健康狀況、家族病史和中風風險
• 進行臨床和實驗室篩查以評估風險因素
• 使用磁共振成像對大腦進行影像篩查,使用磁共振血管造影對腦內和頸部血管進行影像篩查
• 適用於每個人的風險因素控制干預
- 生活方式改善(例如飲食建議和體重管理,戒菸建議等)
- 醫學治療(用於血壓、膽固醇、糖尿病的血糖控制等)
• 神經外科內血管管理(例如顱內或顱外血管異常,頸動脈狹窄等)
針對每個病人進行的篩查促進中風預防和早期干預。採用積極主動的方法來識別中風的風險,包括使用診斷性影像技術識別血管異常、狹窄和現有病變,並根據需要提供相應的干預措施。亞洲醫學專科醫院提供全面的中風篩查,協助家庭醫生對每位病人進行持續管理。
中風:新概念與護理
大多數中風是由於腦部動脈阻塞而引起的急性缺血性中風。在香港,估計約70%的中風是缺血性中風,其餘是出血性中風。中風是一種異質性疾病,兩種中風類型的治療策略不同。重要的是,在干預的每個階段為每個患者提供量身定制的護理,以滿足個人的需求[5]。
過去十年中中風護理的主要發展是認識到急性缺血性中風是一種醫療緊急情況,並且“時間就是腦部”(請見方框特點)[7]。這與使用靜脈內重組組織型纖溶酶原激活劑(rtPA)對缺血性中風進行溶栓治療的可行性相吻合。最近的進展還包括經皮腦血管介入(神經PCI)。這些治療方法在亞洲醫學專科醫生處提供,旨在最大程度地減少中風的殘疾,改善急性缺血性中風患者的結果。
時間就是腦(Time is Brain)。
急性缺血性中風是一種醫療緊急情況。
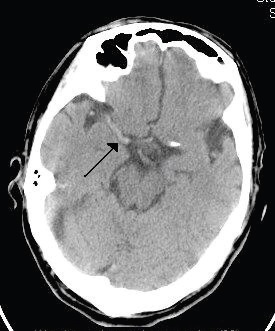 Middle cerebral artery occlusion (arrow). Urgent intervention is essential to prevent rapid and irretrievable loss of nervous tissue. |
需要進行急性缺血性中風的緊急評估和治療。每單位時間內的腦損失估計凸顯了中風護理的時間緊迫性。
- 最常見的缺血性中風類型是大血管、顱內中風。這些中風通常在6至18小時內發展。在中風發展過程中,每小時估計損失1.2億個神經元、8300億個突觸和714公里的髓鞘纖維(表2)。
- 與衰老時正常神經元損失的速率相比,缺血性腦組織在中風發展的每小時會增加3.6年的衰老速度,除非接受治療。
| 表2.急性缺血性中風:預計在沒有及時干預的情況下,神經組織損失的速率。 | |||
| 神經元損失 | 突觸損失 | 髓鞘纖維損失 | |
| 每秒 | 3.2萬 | 2.3億 | 200 米 |
| 每分鐘 | 1.9 百萬 | 140億 | 12 公里 |
| 每小時 | 1.2億 | 8300億 | 714 公里 |
| 每次中風 | 12 億 | 8300兆 | 7140 公里 |
- Source: Saver JL. Stroke.2006;37:263-266.
- Community stroke recognition and response
- A critical step in improving stroke outcomes is ensuring that there is prompt recognition of stroke and rapid access to appropriate treatment facilities. This is essential to ensure patients receive treatment within the therapeutic window for appropriate treatments [8].
Delays in seeking medical attention after stroke/TIA reflect that the patient and those with them fail to recognise the symptoms of stroke/TIA or to seek emergency medical care [9]. The need for greater public awareness is recognised, particularly for those at increased risk of stroke. Through stroke screening, public awareness can be promoted.
The FAST mnemonic (face, arm speech, time) has been shown to identify almost 90% of cases of acute stroke and TIA, with better performance for ischaemic than haemorrhagic stroke [9]. The FAST mnemonic has been used in public awareness campaigns around the world. See the box feature for further details of the FAST. - Recognise stroke symptoms F.A.S.T.
- You can recognise a stroke using the FAST test
FACIAL weakness: Can the person smile? Has their mouth or eye drooped?
ARM weakness: Can the person raise both arms?
SPEECH problems: Can the person speak clearly and understand what you say?
TIME to call for emergency medical help: 24-hour emergency hotline +852 3420 6660
If a person fails any one of these tests, get help immediately by dialling 999
A speedy response can help reduce the damage to a person’s brain and improve their chances of a full recovery. A delay in getting help can result in death or long-term disabilities.
Don’t ignore temporary symptoms.
If symptoms disappear within 24 hours, the person may have had a transient ischaemic attack (TIA), which is also called a mini-stroke. A TIA is still a medical emergency, because it can lead to a major stroke. - 3 Golden hours: Benefits and limitations of intravenous rtPA
- Intravenous rtPA is a proven, established treatment for acute ischaemic stroke 10,11 and is recommended in local and international guidelines for acute stroke treatment [4,5,12]. It needs to be delivered in a well-equipped centre with relevant expertise to allow rapid assessment, investigation, treatment & monitoring 12. Accepted indications for use of this treatment are as presented in Table 3.
The therapeutic benefit of IV rtPA is strongly time-dependent and is greatest when given early after stroke onset and declines over 3 to 4.5 hours. Studies have shown that starting this treatment within 90 minutes of stroke onset is optimum and that for every 10 minute delay within the 1-3 hour treatment time period, 1 fewer patient has an improved disability outcome 10. This has led to initiatives aimed at achieving thrombolysis - so-called ‘door to needle’ times - of within 60 minutes. The American Heart Association/American Stroke Association is currently promoting a goal of 50% of patients with ischaemic stroke having a door to needle time of ≤60 minutes [13].
Key strategies identified to meet this goal include:
• Emergency medical service pre-notification
• Activating the stroke team with a single call
• Rapid access to and interpretation of brain imaging
• Specific protocols and tools for acute stroke management
• A team-based approach. - Symptomatic intracranial bleeding is a recognised and serious side effect of IV rtPA and is estimated to affect approximately 6% of patients [11]. Salvage neurosurgery is a difficult undertaking if intracranial bleeding occurs but is an option in specialist neurosurgical centres, such as the Asia Medical Specialists.
| Table 3. Patient Selection Criteria for IV rtPA [12] |
| Indications |
| • Onset of ischaemic stroke within the preceding 3 hours • Measurable and clinically significant deficit on National Institute of Health Stroke Scale (NIHSS) examination • Patient’s brain imaging does not show haemorrhage or non-vascular cause of stroke • Patient’s age is >18 years |
| Contraindications [14] |
| • Age < 18 • CT scan findings (intracranial hemorrhage, or major acute infarct signs) • Suspicion of subarachnoid hemorrhage (even if head CT is negative for hemorrhage) • Recent (within 3 months) major surgery or trauma (discuss with Attending) • History of intracranial haemorrhage or brain aneurysm or vascular malformation or brain tumor (May consider IV tPA in patients with CNS lesions that have a very low likelihood of haemorrhage, such as small unruptured aneurysms or benign tumors with low vascularity) • Known bleeding diathesis OR 1. Current use of oral anticoagulants with INR > 1.7 or PT > 15 seconds 2. Use of blood thinner within 48 hours preceding onset of stroke AND prolonged aPTT at time presentation 3. Platelets <100,000 4. Internal hemorrhage (GI hemorrhage, urinary tract haemorrhage) < 3 weeks 5. Dabigatran use in the past 48 hours (if last dose >48 hours, confirm normal renal function [creatinine clearance >50 mL/min] and normal coagulation [aPTT, INR, platelet count] before tPA administration). 6. Low molecular weight blood thinner use in the past 24 hours. • Persistent systolic BP >185 mm Hg or diastolic BP >110 mm Hg despite treatment. |
- Source: http://www.bmc.org/stroke-cerebrovascular/services/acute-stroke-protocol.htm
- 8 Golden hours: Neurointerventional techniques for acute ischaemic stroke
- Neuro-PCI
• Intra-arterial thrombolysis (ia rtPA)
• Mechanical thrombectomy
• Intravascular stenting
These treatments can be offered in highly specialised centres with advanced imaging and neurosurgical specialisation. They may be used alone or in combination. A major advantage of these treatments is that they are of benefit beyond the period that intravenous rtPA thrombolysis is effective. They extend the therapeutic window for acute ischaemic stroke treatment from 3 hours, offering up to ‘8 Golden hours’.
Neuro-PCI treatment depends on detailed brain angiography to look for the causative vascular occlusive lesion that PCI will target. The use of neuro-PCI for stroke is similar to the use of cardiac PCI for acute coronary ischaemia. In the United States, comprehensive stroke centres with a vascular neurosurgical service may prefer neuro-PCI over intravenous rtPA treatment because of the reduced risk of bleeding complications. When intra-arterial rtPA is used as part of a neuro-PCI intervention, a very low dose of rtPA is directly infused as an adjunct to mechanical thrombectomy to lyse the blocking thrombus.
Recent data from the MERCI/Multi MERCI trials patients showed that as many as 40% of those who had successful revascularisation with such treatments at 6.9 hours or later after stroke onset still achieved independent functional outcomes [14].
Appropriate treatment should be started as soon as possible after stroke onset for the best outcome. However, in special clinical conditions some patients presenting up to 8 hours after stroke onset, can still benefit from neuro-intervention. - Mechanical thrombectomy
Brain revascularisation can be achieved by mechanical thrombectomy under the fluoroscopic guidance of cerebral angiograms. There are a range of clot retrieval devices that can potentially be used for mechanical thrombectomy [15].
With clot retrieval devices, a guidewire and micro-catheter is passed up to the occluding clot in the intracranial vessel. The thrombus or embolus is then removed by the device using mechanical breakage and aspiration. Clot retrieval devices, such as the MERCI Retrieval System (Concentric Medical Inc., California, USA) (see Fig. 2) have been the most well-researched 15 and the MERCI system has now been in use in the USA and Europe for several years 16. A systematic review of 23 small observational studies found that those treated with clot removal devices were about 15 times more likely to have a good outcome (modified Rankin score ≤2) and 2.2 times less likely to die [15].
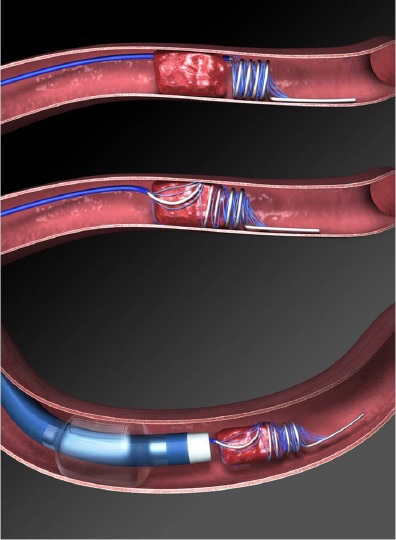 Fig. 2 The MERCI Clot Retriever for mechanical thrombectomy |
- The Penumbra System (Penumbra, Alameda, California, USA) 16 is a more recent device also designed for use in acute ischemic stroke secondary to large vessel hromboembolism (Fig. 3).
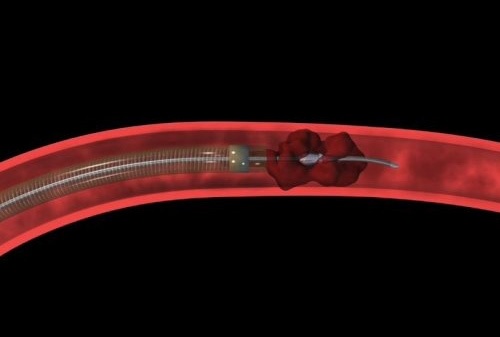 Fig. 3 The Penumbra System for mechanical thrombectomy |
- Intra-arterial thrombolysis
Injection of IA rtPA at the site of the thromboembolism improves outcomes in acute ischaemic stroke. A Cochrane review found that IA thrombolysis resulted in a significant reduction in the combined odds of death and dependency at follow-up [11].
Use of intravascular stents
With advances in endovascular stent design and delivery, stenting has recently become a feasible treatment option for neurovascular disease [17]. Stents initially conceived for treatment of intracranial atherosclerosis (Wingspan stent) and for aneurysm remodelling (Enterprise and Neuroform stents) have paved the way for new therapeutic approaches in acute ischaemic stroke [18].
Clinical studies to date have shown that stents are efficacious in the treatment of acute ischaemic stroke [17].
Intravascular stents can be deployed as part of neuro-PCI if there is concomitant vascular stenosis.
| Potential advantages of neuro-PCI | |
| Neuro-PCI | Intravenous rtPA |
| Extends the therapeutic window from 3 hours up to 8 hours. Neuro-PCI offers a treatment option for those with acute stroke who do not access specialist medical services within 3 hours. Effective neuro-PCI revascularisation in the 4th to 7th hour may salvage brain cells in the Penumbra Zone (peripheral ischaemic region) minimising the area of infarction. | Accepted therapeutic window for treatment is 3 hours. Studies show optimum use is within 90 minutes [10]. These time-to-treatment intervals have proved generally difficult to achieve due to patient factors, lack of community awareness and access and provision of appropriate medical services. |
| Neuro-PCI may be suitable for individual patients who: a) have a contraindication to intravenous rtPA; or b) have not had an adequate therapeutic response to intravenous rtPA. | Symptomatic intracranial bleeding is a recognised and serious side effect of IV rtPA and is estimated to affect approximately 6% of patients [11]. |
| Intra-arterial delivery of lytic agents may increase the chance of recanalisation. | Occlusions in some areas (e.g. proximal middle cerebral artery) are known to be more resistant to intravenous delivery of lytic agents [19]. |
- Summary
- Stroke is a brain attack and time is brain.
Prevention through screening and risk factor control is the best possible treatment.
Awareness of stroke symptoms and rapid access to emergency medical care is necessary to improve outcomes.
Neurointervention techniques now allow effective acute ischaemic stroke treatment for up to a GOLDEN 8 HOURS. - References
- 1. Strong K, Mathers C, Bonita R. Preventing stroke: saving lives around the world. The Lancet Neurology. 2007;6:182-7.
2. Ng PW. The stroke epidemic. Hong Kong Med J 2007;13:92-4.
3. National Stroke Association. Stroke facts. http://www.stroke.org Accessed 26 June 2012.
4. Schwamm L, Fayad P, Acker JE III, Duncan P, Fonarow GC,Girgus M. Translating evidence into practice: a decade of efforts by the American Heart Association/American Stroke Association to reduce death and disability due to stroke: A Presidential advisory for the American Heart Association/American Stroke Association. Stroke 2010;41:1051-65.
5. Ng PW, Huang CY, Cheung RTF, Wong KS, Wong CK, Lam JK for the Hong Kong Neurological Society and Hong Kong Stroke Society. Consensus statement on ischaemic stroke care in Hong Kong. Hong Kong Med J 2004;10:124-9.
6. O’Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al: INTERSTROKE investigators. Risk factors for ischaemic and intracerebral aemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010;10:112-23.
7. Saver JL. Time is brain – quantified. Stroke 2006;37:263-266.
8. Kleindorfer DO, Miller R, Moomaw CJ, Alwell K, Broderick JP,Khoury J, et al. Designing a message for public education regarding stroke. Does FAST capture enough stroke? Stroke 2007;38:2864-2868.
9. Sprigg N, Machilli C, Otter ME, Wilson A, Robinson TG. A systematic review of delays in seeking medical attention after transient ischaemic attack. J Neurol Neurosurg Psychiatry 2009;80:871-5.
10. Fonarow GC, Smith EE, Saver JL, Reeves MJ, Bhatt DL, Grau-Sepulveda MV, et al. Timeliness of tissue-type plasminogen activator therapy in acute ischaemic stroke. Circulation 2011;123:750-758.
11. Wardlaw JM, Murray V, Berge E, del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Reviews. 2009. CD000213.
12. National Stroke Foundation (Australia). Clinical Guidelines for Stroke Management 2010. Melbourne, Australia. www.strokefoundation.com.au
13. Fonarow GC, Smith EE, Saver JL, Reeves MJ, Hernandez AF, Peterson ED, et al. Improving door-to-needle times in acute ischaemic stroke. The design and rationale for the American Heart Association/American Stroke Associations’s Target: Stroke initiative. Stroke 2011;42:2983-2989.
14. Nogueira PC, Smith WS, Sung G, Duckwiler G, Walker G, Roberts R, et al. Effect of time to reperfusion on clinical outcome of anterior circulation strokes treated with thrombectomy. Stroke 2011;42:3144-3149.
15. Stead LG, Gilmore RM, Bellolio MF, Rabinstein AA, Decker WW. Percutaneous clot removal devices in acute ischaemic stroke: A systematic review and meta-analysis. Arch Neurol 2008:65:1024-30.
16. Bose A, Henkes H, Alfke K, Reith W, Mayer TE, Berlis A, Branca V, Po Sit S, for the Penumbra Phase I Stroke Trial Investigators. The Penumbra System: A mechanical device for the treatment of acute stroke due to thromboembolism. AJNR 2008;29:1409-1413.
17. Ansari S, McConnell DJ, Velat GJ, Waters MF, Levy EI,Hoh BL, et al. Intracranial stents for treatment of acute ischaemic stroke: evolution and current status. World Neurosurg 2011;76:S24-34.
18. Samaniego FA, Dabus G, Linfante I. Stenting in the treatment of acute ischemic stroke: literature review. Front Neurol 2011;2:76. Epub 2011 Dec 9.
19. Meyers PM, Schumacher C, Sander Connolly E, Heyer EJ, Gray WA, Higashida RT. Current status of endovascular stroke treatment. Circulation 2011;123:2591-2601.
| Copyright ©2017 Asia Medical Specialists Limited. All rights reserved. |
